Adult
- About
- Meet The Team
- Conditions
- Anticoagulation in Pregnancy
- Aortic Dilatation and Pregnancy
- Aortic Valve Disease
- Aortic Valve Replacement
- Atrial Septal Defect
- Coarctation - Transcatheter stent (keyhole) treatment
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Ebsteins Anomaly
- Eisenmenger’s Syndrome
- Fontan Circulation
- Mitral Valve Repair/Replacement
- Normal Heart
- Patent Foramen Ovale
- Pregnancy information for women with metal heart valves
- Pulmonary Incompetence
- Pulmonary Stenosis
- Pulmonary Valve Replacement - Surgery
- Pulmonary valve replacement - Transcatheter (keyhole) treatment
- Repaired Atrioventricular Septal Defects
- Sub-aortic Stenosis
- Surgical treatment of Atrial Septal Defect
- Tetralogy of Fallot
- Transposition of the Great Arteries - The Atrial Switch (Mustard or Senning) procedure
- Transposition of the Great Arteries – Arterial Switch
- Ventricular Septal Defect
- Ventricular Septal Defect - Transcatheter (keyhole) treatment
- Patient Feedback
- Making the most of your clinic appointment
- Your Appointment in Outpatients
- Easy Read Guide for Out Patients
- Cardiac Catheter
- Transoesophageal Echocardiogram
- MRI
- Surgery & "Top Tips" for coming into hospital
- Lifestyle Advice
- Exercise
- Heart Failure
- End of Life and Palliative Care
- Looking after your oral health
- Dentists Information Section: Dental care in adults at risk of Infective Endocarditis
- Yorkshire Regional Genetic Service
- Support
- Video Diaries
- Second Opinion
- Monitoring Results at Leeds Infirmary
- Professionals
Coarctation - Transcatheter stent (keyhole) treatment
A coarctation is a narrowing in the main blood vessel in the body (the aorta). The aorta carries oxygenated blood from the heart to the rest of the body. The narrowing acts like a dam causing high blood pressure in the top half of the body and reducing blood flow to the rest of the body.
This condition is usually picked up in childhood, but is occasionally diagnosed for the first time in adult life, usually because someone is found to have high blood pressure.
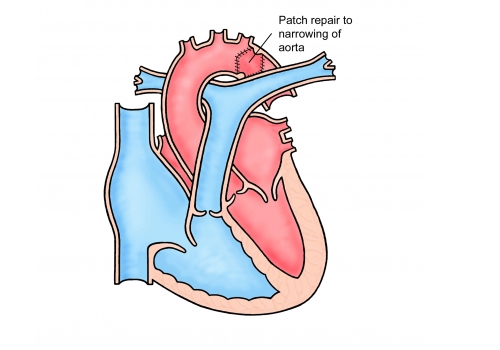
Why does my coarctation need treating?
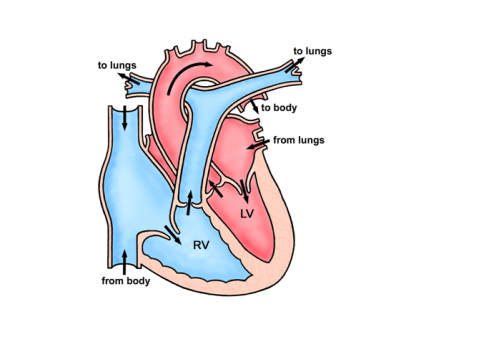
Unrepaired narrowings (coarctations) place strain on the main pumping chamber of the heart (the left ventricle – see picture above) and lead to high blood pressure. Untreated, both of these complications can significantly shorten a patient’s life. High blood pressure is related to stroke and heart attack.
What are the options for treatment?
Many coarctations are picked up in early childhood where surgery is the best treatment option. In teenage and adult patients some narrowings can be technically very difficult to repair using open surgery and can require lengthy operations.
In some patients, the narrowing is not discovered until they are much older or re-narrowing can occur due to scarring at the site of a previous operation. In these patients it is possible in some (but not all) cases to stretch the narrowing using a keyhole technique. Many patients who are diagnosed with a coarctation in adulthood will be offered a stent procedure to open the narrowing. You may need a CT or MRI scan to see if you are suitable for this.
What are the advantages of keyhole treatment?
The main advantage of the keyhole technique is that it avoids an operation which leaves a scar on the side of the chest that can be painful afterwards for a number of weeks. The keyhole technique is performed as an overnight procedure whereas surgery requires a short stay on the intensive care unit followed by about a week in hospital. There are other less serious complications of a major operation and a hospital stay (wound infections, potential for blood clots in the leg etc) which are avoided by the keyhole approach.
Keyhole treatment is now generally considered first line treatment for adults with coarctation of the aorta.
What are the risks of keyhole treatment for coarctation?
• The risk of death during the procedure is less than 1 in 100.
• Migration (movement) of the stent (metal cage) can occur during the procedure (2%). Generally, a migrated stent can be safely repositioned but in some cases may require an operation to remove it.
• Aneurysm (blow out of the blood vessel) can occur and can require further treatment.
• Stroke can occur in less than 1% of patients
• Damage to the leg artery (which is used to put the stent in) requiring treatment occurs in approximately 4% (1/20) patients
How is the procedure performed?
The procedure is performed under general anaesthetic. A tube is inserted into the artery at the top of the leg and pictures are taken. A balloon with a metal cage (stent) on the outside is inserted into the tube in the artery and positioned across the narrowing. The balloon is inflated and the stent stays in position holding open the narrowed area (see picture below).
After the procedure the tubes are removed and the hole in the artery is closed using an automatic stitch device.What happens after the procedure?
If there are no problems you will go home the following day. Your leg may be sore for a week and there may be some bruising. Follow up will be arranged in the cardiology clinic and usually an MRI scan is performed around 3 months after the procedure to check for any weakness (aneurysm) of the vessel wall as a result of the procedure.
Most people do not need longer than a week off work. You should avoid any heavy lifting/strenuous exercise for 3-4 days until your leg is no longer sore.
You shouldn’t have any worrying side effects or symptoms but if you do you can telephone the specialist nurses for advice during the week (8am-4pm) or 111 out of hours. You will be given specific advice regarding what to look out for when you are discharged from hospital.
Follow up will include reviews with a cardiologist and usually an MRI scan every 3-5 years.
Do I have a choice?
A small number of patients will decide they do not want any form of treatment at all having understood all the risks. If this is the case, we would still encourage you to come for regular reviews.
Other information
If you decide to proceed you will be placed on the waiting list. When you are given a date for your procedure you will also be given a date for your pre-assessment clinic appointment which will be 2-3 weeks in advance of your procedure. At this appointment you will have some routine tests including blood tests.
You will receive a letter through the post with your procedure date and with your pre-assessment date. We try to give you around 4 weeks’ notice but it’s often not possible for us to give you more than a week or two notice of the date of your procedure. Please contact the secretary as soon as you receive your letter to confirm on 0113 3928184 or
leedsth-tr.paedcardcathlist@nhs.net .
This is very important, if you do not confirm in good time your slot will be offered to someone else.
If you are taking anticoagulant (blood thinning) drugs such as warfarin or rivaroxaban you will need to stop this in advance. This will be discussed with you at pre-assessment.
Please make sure you have had a recent dental check-up and all outstanding dental treatment has been completed before the procedure due to the small risk of endocarditis (infection in the heart).