Adult
- About
- Meet The Team
- Conditions
- Anticoagulation in Pregnancy
- Aortic Dilatation and Pregnancy
- Aortic Valve Disease
- Aortic Valve Replacement
- Atrial Septal Defect
- Coarctation - Transcatheter stent (keyhole) treatment
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Ebsteins Anomaly
- Eisenmenger’s Syndrome
- Fontan Circulation
- Mitral Valve Repair/Replacement
- Normal Heart
- Patent Foramen Ovale
- Pregnancy information for women with metal heart valves
- Pulmonary Incompetence
- Pulmonary Stenosis
- Pulmonary Valve Replacement - Surgery
- Pulmonary valve replacement - Transcatheter (keyhole) treatment
- Repaired Atrioventricular Septal Defects
- Sub-aortic Stenosis
- Surgical treatment of Atrial Septal Defect
- Tetralogy of Fallot
- Transposition of the Great Arteries - The Atrial Switch (Mustard or Senning) procedure
- Transposition of the Great Arteries – Arterial Switch
- Ventricular Septal Defect
- Ventricular Septal Defect - Transcatheter (keyhole) treatment
- Patient Feedback
- Making the most of your clinic appointment
- Your Appointment in Outpatients
- Easy Read Guide for Out Patients
- Cardiac Catheter
- Transoesophageal Echocardiogram
- MRI
- Surgery & "Top Tips" for coming into hospital
- Lifestyle Advice
- Exercise
- Heart Failure
- End of Life and Palliative Care
- Looking after your oral health
- Dentists Information Section: Dental care in adults at risk of Infective Endocarditis
- Yorkshire Regional Genetic Service
- Support
- Video Diaries
- Second Opinion
- Monitoring Results at Leeds Infirmary
- Professionals
Coarctation of the Aorta
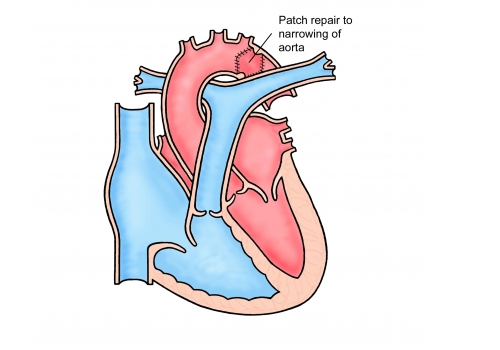
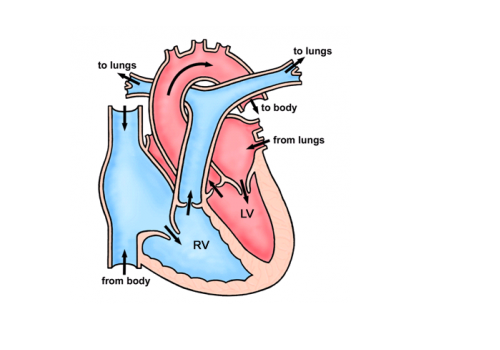
Coarctation of the aorta is a condition where there is a narrowing of the aorta – the main blood vessel which carries blood from the heart to the rest of the body. This narrowing acts like a dam causing high blood pressure in the top half of the body and reducing blood flow to the rest of the body.
Here’s a video explaining about Coarctation
Here’s a video about the treatment of Coarctation
This condition is usually picked up in childhood, but is occasionally diagnosed for the first time in adulthood, usually because someone is noted to have high blood pressure.
Treatment in childhood
If your coarctation was picked up in childhood it will usually have been treated with an operation, involving either removal of the narrowed segment or widening the narrowing by insertion of a patch of either Gore-Tex or part of the wall of another artery. These operations are mostly done through the side of your chest and have very good long term outcomes.
Follow up in adult life
We recommend that everybody who has had a coarctation repair is followed up lifelong. This is because we do see the following problems in some patients;
- High blood pressure – we know that if you had a coarctation repair in childhood you have a higher chance of developing high blood pressure at an earlier age – this can lead to early heart disease or stroke
- Re-narrowing at the site of the previous coarctation – the material used to repair the coarctation may not have expanded as you grew – therefore some patients develop re-narrowing and some require further treatment for this
- Aneurysm formation – some patients develop a weakness and swelling of the aortic wall at the site of the previous surgery
- Aortic valve problems – many patients with coarctation of the aorta also have abnormalities of the aortic valve (main outlet valve of the heart)
We usually recommend that you have an MRI scan of your aorta when you transfer from paediatric to adult services. These are repeated around every 3 -5 years depending on what we see on the first scan. We also often use 24 hour blood pressure monitors to see exactly what is happening with your blood pressure.
Treatment in adult life
If you are found to have a coarctation in adult life you will be assessed to see if it is suitable for treatment either by surgery or by a keyhole technique. If you have had a previous coarctation repair and we find it is re-narrowed and you have high blood pressure we will discuss with you whether you should have further treatment. This will be either by taking tablets, further surgery or a keyhole procedure.
Important points to consider
- Exercise: Regular exercise, to a moderate level, is encouraged. It is good for overall health and can also help to keep blood pressure lower / under control. Activities such as walking, cycling, and swimming are ideal and it is important to warm up and warm down slowly. It is best to avoid really intense cardiovascular exercise, for example distance running, or sudden ‘bursts’ of strenuous activity. Heavy weight lifting should be avoided, but it is usually okay to go to do low level weights at the gym (up to 15kg), ensuring that you are able to do 3 sets of 12-15 repetitions without any strain/breath-holding. Other activities that cause you to hold your breath or strain to lift/move objects, for example shovelling snow, trying to push a heavy object or playing some brass/woodwind instruments should be avoided as these can raise your blood pressure too much
- Remember it’s important to come for your review appointments
- Look after your teeth. You no longer need antibiotic cover for any dental work or non-sterile surgical procedures. Regular dental checks every 6-12 months are recommended.
- Do have your blood pressure checked in the RIGHT arm only. The blood pressure in your left arm is likely to be falsely low.
- Talk to us before you get pregnant. This is to enable the cardiologist to assess your heart in more detail prior to pregnancy and to arrange further tests if necessary. The chances of having a baby born with congenital heart disease are slightly increased from the general population if you have congenital heart disease yourself. The risk is generally quoted as being about 2-4%, compared to 1% for the general population. Your cardiologist can discuss this with you in clinic prior to planning a family. We can offer a specialised scan of your unborn baby’s heart at 18-20 weeks, which can detect any major abnormality of the heart.
Adult Congenital Heart Team
Leeds General Infirmary