Adult
- About
- Meet The Team
- Conditions
- Anticoagulation in Pregnancy
- Aortic Dilatation and Pregnancy
- Aortic Valve Disease
- Aortic Valve Replacement
- Atrial Septal Defect
- Coarctation - Transcatheter stent (keyhole) treatment
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Ebsteins Anomaly
- Eisenmenger’s Syndrome
- Fontan Circulation
- Mitral Valve Repair/Replacement
- Normal Heart
- Patent Foramen Ovale
- Pregnancy information for women with metal heart valves
- Pulmonary Incompetence
- Pulmonary Stenosis
- Pulmonary Valve Replacement - Surgery
- Pulmonary valve replacement - Transcatheter (keyhole) treatment
- Repaired Atrioventricular Septal Defects
- Sub-aortic Stenosis
- Surgical treatment of Atrial Septal Defect
- Tetralogy of Fallot
- Transposition of the Great Arteries - The Atrial Switch (Mustard or Senning) procedure
- Transposition of the Great Arteries – Arterial Switch
- Ventricular Septal Defect
- Ventricular Septal Defect - Transcatheter (keyhole) treatment
- Patient Feedback
- Making the most of your clinic appointment
- Your Appointment in Outpatients
- Easy Read Guide for Out Patients
- Cardiac Catheter
- Transoesophageal Echocardiogram
- MRI
- Surgery & "Top Tips" for coming into hospital
- Lifestyle Advice
- Exercise
- Heart Failure
- End of Life and Palliative Care
- Looking after your oral health
- Dentists Information Section: Dental care in adults at risk of Infective Endocarditis
- Yorkshire Regional Genetic Service
- Support
- Video Diaries
- Second Opinion
- Monitoring Results at Leeds Infirmary
- Professionals
Atrial Septal Defect
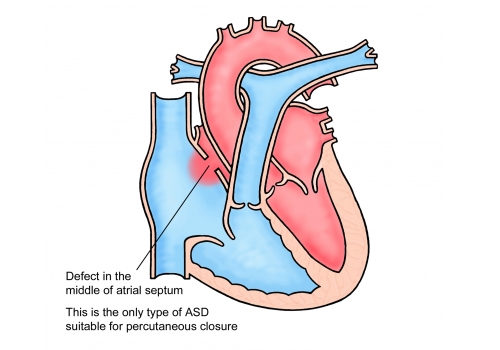
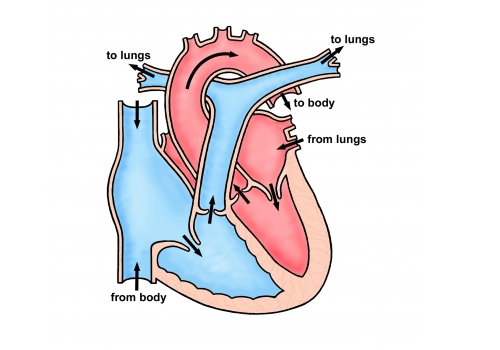
An atrial septal defect (or “ASD”) is a hole between the two smaller collecting chambers of the heart. It allows blood to cross from the left chamber to the right leading to extra flow through the lung artery. Usually patients with ASD’s have very few symptoms but eventually, during later adult life breathlessness and electrical instability of the heart can develop.
There are three types of ASD’s:
Watch this video to see how an ASD affects the heart.
Secundum ASD. This is the most common ASD, affecting around 90% of people with ASD’s. It is caused when part of the atrial septum does not close whilst the heart is developing. This results in a hole in the middle of the wall separating the two atria.
Sinus Venosus ASD. This defect is in the upper part of the atrial septum, near where a large vein (the superior vena cava) brings oxygen-poor blood from the upper body to the right atrium. Sinus venosus defects are rare, and they don’t close on their own. Sometimes the veins carrying blood back to the heart from the lungs can be abnormal in that the veins drain into the right atrium, rather than the left atrium. In nearly all cases these are treated by open heart surgery.
Primum ASD. This defect occurs in the lower part of the atrial septum and often is associated with mitral and tricuspid heart valve problems.
Will my defect need closing?
We would generally recommend closure of all but the smallest of ASD’s, unless other problems are present that would make this unwise (for example damage to the lungs, which can occur in some patients with ASD’s). Your cardiologist will make an assessment of the hole in your heart and any other problems you have and discuss treatment with you.
Treatment
There are two options:
1) Surgery
Have a look at the video about to see about ASD surgery.
ASD’s were among the first heart abnormalities to be treated with an operation in the 1950’s. Surgery involves opening the chest through the breast bone and taking over the function of the heart and lungs with a machine (“heart bypass”) to allow the surgeon to stop the heart, and repair the hole with stitches and a patch. The procedure is very safe with a risk of dying of around 1 in 300. There is an even smaller risk of brain damage (stroke) related to the use of the bypass machine. Other problems can occur, such as fluid collecting around the heart or temporary electrical instability but these are rarely serious. After surgery a short stay on the intensive care unit (usually around a day) and then a period in hospital for observation (usually about 5 days) is required before going home. Opening the front of the chest leads to a scar and the chest wall will be sore whilst it heals. The time taken to get fully back to normal varies from person to person but can be up to 3 months.
2. Keyhole treatment
Closure of ASD’s using a “keyhole” technique has been performed in large numbers of patients (over 100,000) since the mid 1990’s. There are a number of devices available and they are usually made from a mixture of fine wire and synthetic cloth. The devices fold into a thin tube (catheter) which is inserted into the vein in the groin under general anaesthetic. The device is then unfolded into the hole and released. The device stays in the heart and eventually becomes covered by your own tissue during the healing process.
Potential advantages of keyhole treatment over surgery are that it avoids the scar on the chest and the discomfort of an operation. The stay in hospital is usually one night and there is no need for intensive care. Comparisons of surgery and keyhole treatment generally show that keyhole treatment is just as good at “treating” the hole in the longer term. Complications are rare and are different to those that happen after open heart surgery.
Risks of keyhole closure
There have now been sufficient implants worldwide for us to compare keyhole closure with surgery. Keyhole treatment is not suitable for all ASD’s. Although your cardiologist will make a careful assessment of your suitability for keyhole treatment it is not until you are asleep under anaesthetic and a detailed scan (trans-oesophageal echo or “TOE”) is done that we can be absolutely sure. There is a small chance that you may go for the keyhole procedure and be woken from the anaesthetic with the hole still present if the cardiologist is unable to close it (overall this happens in about 1 in 10 cases).
The risk of death with keyhole treatment is around 1 in 1000. There is a small risk of brain damage (less than for the surgical alternative). The device can fall out at the time of implant or shortly after (in Leeds, about 1 in 100 cases). Sometimes, in this situation the device can be “lassoed” with a special catheter (tube) and retrieved but often an open heart operation is required to get the device back and close the hole. Occasionally a residual hole can be left after closure with a device and if this is large then surgery may be needed to close it.
There is a very small risk (around 2 per 100 cases) of cardiac erosion. This is when the device damages the walls of the heart in the longer term. This is a very rare but serious complication and in most cases, happens within the first year but can sometimes be a later complication. There is nothing you can do to reduce this risk. Symptoms of erosion may include chest pain, numbness, sudden weakness, dizziness, fainting, shortness of breath or a rapid heartbeat. If you experience those symptoms after a device closure you should contact your doctor.
Will I get any side effects?
Groin tenderness and bruising is the most common side effect and is completely normal. You will be given specific discharge advice from hospital about what to look out for in regards to your groin wound.
Sometimes, people experience headaches or migraine following keyhole closure of their ASD. If you had migraine before the procedure it can get better after the ASD is closed-no one knows why this is the case for sure but headaches rarely remain a problem beyond a few months after implant once the device has sealed in the heart. If you do get headaches paracetamol or ibuprofen are fine to take. Sometimes people need specific migraine medication from their pharmacy or GP.
Sometimes people experience palpitations after their procedure. Again, this should settle down with time but if you have any palpitations that make you feel unwell and do not go away you should seek advice from the specialist nursing team during the week (8am-4pm) or 111 out of hours. If you have palpitations that make you feel very unwell you should call 999 or go to A&E.
Occasionally people develop irregular heart rhythms. This can usually be treated and does not return. Sometimes the irregular heart rhythm does not go away and it is managed with medication long-term. This is more likely to happen if you have had an irregular heart rhythm before the procedure.
Other advice and practicalities
For those patients undergoing keyhole treatment we advise treatment with aspirin (and sometimes another similar drug called Clopidogrel) for around 6 months after closure.
Most people do not need longer than a week off work. You should avoid any heavy lifting/strenuous exercise for 3-4 days until your leg is no longer sore.
Most people will remain well and lead a completely normal life after ASD closure. No restrictions to physical activity are required.
Most people who are attending for keyhole ASD closure do not need to attend a pre-assessment clinic. If you have a lot of other health problems then we may require you to attend pre-assessment or we may arrange some routine blood tests at your GP practice.
If you are taking an anticoagulant drug (blood thinner) this should be stopped in advance (usually around 3 days). A nurse will contact you to advise upon this around a week in advance of the procedure.
Please make sure you have had a recent dental check-up and all outstanding dental treatment has been completed before the procedure due to the small risk of endocarditis (infection in the heart).
You will receive a date for your procedure through the post. We try to give you around 4 weeks’ notice but it’s often not possible for us to give you more than a week or two notice of the date. Please contact the secretary as soon as you receive your letter to confirm on 0113 3928184 or leedsth-tr.paedcardcathlist@nhs.net .
This is very important, if you do not confirm in good time your slot will be offered to someone else.
If you receive the date for your procedure and become unwell, or something has changed since your clinic appointment, please contact the specialist nursing team who will advise whether any further tests are necessary.
We appreciate it can be quite a wait between your clinic appointment and your procedure so, if in the time waiting for your procedure you have any questions or concerns, then please contact the specialist nursing team who will be happy to assist you.