Adult
- About
- Meet The Team
- Conditions
- Anticoagulation in Pregnancy
- Aortic Dilatation and Pregnancy
- Aortic Valve Disease
- Aortic Valve Replacement
- Atrial Septal Defect
- Coarctation - Transcatheter stent (keyhole) treatment
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Ebsteins Anomaly
- Eisenmenger’s Syndrome
- Fontan Circulation
- Mitral Valve Repair/Replacement
- Normal Heart
- Patent Foramen Ovale
- Pregnancy information for women with metal heart valves
- Pulmonary Incompetence
- Pulmonary Stenosis
- Pulmonary Valve Replacement - Surgery
- Pulmonary valve replacement - Transcatheter (keyhole) treatment
- Repaired Atrioventricular Septal Defects
- Sub-aortic Stenosis
- Surgical treatment of Atrial Septal Defect
- Tetralogy of Fallot
- Transposition of the Great Arteries - The Atrial Switch (Mustard or Senning) procedure
- Transposition of the Great Arteries – Arterial Switch
- Ventricular Septal Defect
- Ventricular Septal Defect - Transcatheter (keyhole) treatment
- Patient Feedback
- Making the most of your clinic appointment
- Your Appointment in Outpatients
- Easy Read Guide for Out Patients
- Cardiac Catheter
- Transoesophageal Echocardiogram
- MRI
- Surgery & "Top Tips" for coming into hospital
- Lifestyle Advice
- Exercise
- Heart Failure
- End of Life and Palliative Care
- Looking after your oral health
- Dentists Information Section: Dental care in adults at risk of Infective Endocarditis
- Yorkshire Regional Genetic Service
- Support
- Video Diaries
- Second Opinion
- Monitoring Results at Leeds Infirmary
- Professionals
Ventricular Septal Defect - Transcatheter (keyhole) treatment
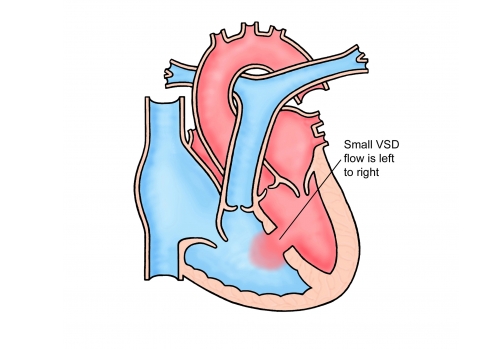
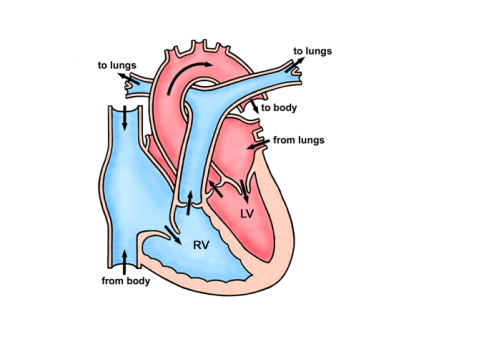
A ventricular septal defect (VSD) is a hole between the two main pumping chambers (ventricles) of the heart. Ventricular septal defects are the second most common cardiac defect, accounting for approximately a fifth of all congenital cardiac anomalies. It allows blood to cross from the left chamber to the right leading to extra blood flow through the lungs. Holes of this kind can occur anywhere along the length of the dividing wall with the majority (80%) occurring “high” up in the septum towards one of the outlet valves of the heart (arrowed in the picture). This sort of defect is known as a perimembranous VSD. Defects lower down towards the bottom of the heart are called muscular VSD’s.
Why does my defect (VSD) need closing?
Most large defects (VSD’s) cause problems related to breathlessness in babies during early life when the only treatment option available is open heart surgery. The majority of smaller defects do not cause symptoms and never require any treatment at all. These defects are simply monitored over the years by a cardiologist. A small number of defects are small enough not to require treatment as a baby but large enough to put strain on the heart over a period of time such that closure of the defect will benefit the patient. There are also circumstances (e.g. if the hole is close to a valve and it causes the valve to leak) where closing the hole is a good idea in the long term. VSD’s can be associated with endocarditis (infection in the heart). If you have a VSD and have had endocarditis we would recommend closure. For some patients the hole can be closed with a plug delivered through a tube (catheter) using a keyhole technique rather than an open heart operation.
What are the advantages of keyhole treatment over open heart surgery?
There are two major advantages of keyhole treatment compared with open heart surgery. Firstly, the procedure avoids a sternotomy (breaking open the breast bone) which leaves a scar and can be painful for a number of weeks after the operation. Secondly, in order to perform an open-heart operation, the surgeon has to stop the heart and stitch the hole closed. To do this a machine takes over the function of the heart (bypass). This process is associated with small complications (brain and other organ damage).
A keyhole procedure avoids both a sternotomy and bypass and also has a much shorter stay in hospital (1 day vs about 5 days), with no time on the intensive care unit and no postoperative pain. Most patients after a keyhole approach will be up and around the same evening and will be able to get back to normal activities within a couple of days.
What are the risks of keyhole VSD closure?
The main side effects include bruising and tenderness at the top of the leg. Before you go home from hospital you will be told what to look out for.
The risk of death or stroke during the procedure is much less than 1 in 100.
There is a small risk of the device dislodging and falling out such that occasionally the device may need to be removed during the same procedure. If it is not possible to retrieve a dislodged device, an open heart operation can sometimes be required to remove the device and close the hole at the same time.
Electrical disturbances can occur during the procedure. Generally, these do not require treatment. There is a small risk of a slow heart rhythm (heart block) related to pressure from the plug on the electrical system in the heart. In some cases, a permanent pacemaker can be needed. At present we do not know the exact risk of heart block as a result of the procedure but it seems to occur in between 1 and 5 % of cases reported in the scientific literature and depends very much on the position of the hole – for some patients there may be no risk at all.
There is a small risk of heart perforation or valve damage (less than 1 in 100) which may need emergency heart surgery.
There is a small risk of a residual leak around the device. Generally, this heals with time but there are rare reports of residual holes not closing and needing further treatment. Occasionally residual holes can cause breakdown of red blood cells that can require another procedure. This is called haemolysis but is rare.
How do you close the hole?
We use a device (plug) made of a metal mesh. The device is called an Amplatzer device but there are other types and shapes of device used for VSD closure as well.
The procedure is carried out under general anaesthetic. Firstly, we perform a TOE (an echo scan from the back of the throat) to get detailed pictures of the hole. There is a small chance that this test may show something that means we cannot close the hole and have to wake you up from the anaesthetic. Catheters (tubes) are then placed in the vessels at the top of the leg and angiograms (pictures) taken of the defect. The defect is then crossed with a long wire and a loop is made across the hole and out of the body. The device is then positioned through a larger delivery tube (see arrow below) and released after safety checks. The whole procedure takes about 2 hours.
For a week before your procedure and around 6 months afterwards it will be necessary to take aspirin (75mg) to prevent small blood clots forming on the device. Sometimes this is needed lifelong. Occasionally another drug is also needed.
Do I have a choice?
Some patients decide that although their hole may be closable with a keyhole technique that they would prefer an open heart operation. A small number of patients will decide they do not want any form of treatment at all having understood all the risks. If you choose not to have your VSD closed, you must take extra precautions to reduce your risk of getting endocarditis (good dental hygiene and regular dental check-ups, avoiding tattoos and piercings, being aware of the signs and symptoms of endocarditis).
Other information
If you decide to proceed with your transcatheter VSD closure, you will be placed on the waiting list. We try to give you around 4 weeks’ notice but it’s often not possible for us to give you more than a week or two notice of the date of your procedure. When you are given a date for your procedure you will also be given a date for your pre-assessment clinic appointment. At this appointment you will have some routine tests including blood tests.
Please contact the secretary as soon as you receive your letter to confirm on 0113 3928184 or
leedsth-tr.paedcardcathlist@nhs.net .
This is very important, if you do not confirm in good time your slot will be offered to someone else.
Most people do not need longer than a week off work. You should avoid any heavy lifting/strenuous exercise for 3-4 days until your leg is no longer sore.
Most people will remain well and lead a completely normal life after VSD closure. No restrictions to physical activity are required.
If you are taking an anticoagulant drug (blood thinner) this should be stopped in advance (usually around 3 days). A nurse will contact you to advise upon this around a week in advance of the procedure.
You will need to take aspirin (and sometimes another similar drug) for 1 week before closure and around 6 months afterwards.
Please make sure you have had a dental check-up and that all outstanding dental work is complete before your VSD closure due to the small risk of endocarditis (infection in the heart). If you have not seen a dentist this may delay your procedure.
We appreciate it can be quite a wait between your clinic appointment and your procedure so, if in the time waiting for your procedure you have any questions or concerns, then please contact the specialist nursing team
who will be happy to assist you.