Adult
- About
- Meet The Team
- Conditions
- Anticoagulation in Pregnancy
- Aortic Dilatation and Pregnancy
- Aortic Valve Disease
- Aortic Valve Replacement
- Atrial Septal Defect
- Coarctation - Transcatheter stent (keyhole) treatment
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Ebsteins Anomaly
- Eisenmenger’s Syndrome
- Fontan Circulation
- Mitral Valve Repair/Replacement
- Normal Heart
- Patent Foramen Ovale
- Pregnancy information for women with metal heart valves
- Pulmonary Incompetence
- Pulmonary Stenosis
- Pulmonary Valve Replacement - Surgery
- Pulmonary valve replacement - Transcatheter (keyhole) treatment
- Repaired Atrioventricular Septal Defects
- Sub-aortic Stenosis
- Surgical treatment of Atrial Septal Defect
- Tetralogy of Fallot
- Transposition of the Great Arteries - The Atrial Switch (Mustard or Senning) procedure
- Transposition of the Great Arteries – Arterial Switch
- Ventricular Septal Defect
- Ventricular Septal Defect - Transcatheter (keyhole) treatment
- Patient Feedback
- Making the most of your clinic appointment
- Your Appointment in Outpatients
- Easy Read Guide for Out Patients
- Cardiac Catheter
- Transoesophageal Echocardiogram
- MRI
- Surgery & "Top Tips" for coming into hospital
- Lifestyle Advice
- Exercise
- Heart Failure
- End of Life and Palliative Care
- Looking after your oral health
- Dentists Information Section: Dental care in adults at risk of Infective Endocarditis
- Yorkshire Regional Genetic Service
- Support
- Video Diaries
- Second Opinion
- Monitoring Results at Leeds Infirmary
- Professionals
Ebsteins Anomaly
This information explains about the condition Ebsteins anomaly, and surgery related to the tricuspid valve that may be suitable for some patients
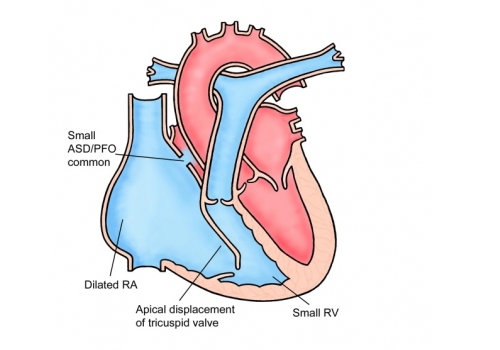
What is it?
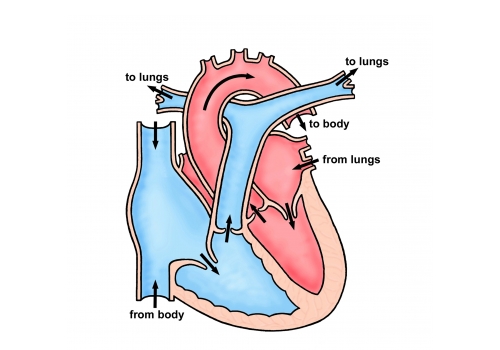
Ebsteins anomaly is an abnormality of the tricuspid valve in which the valve is abnormal and leaks and is displaced towards the point of the heart. There is often a small hole in the heart too, and many people with Ebsteins anomaly also have serious or troublesome heart rhythm problems. Ebsteins anomaly varies from very mild forms of the condition to very severe forms. The treatments usually depend on how badly affected your heart is by the Ebsteins anomaly.
What symptoms may I get?
You may feel more breathless and tired than your peers when you exercise. Some patients leak a little blue blood across the hole in their heart causing them to go a little blue when they exercise. This can also increase your risk of a stroke. Many patients will have palpitations (a feeling of your heart race or bump). Some very severely affected patients develop swelling of the abdomen and legs.
What treatments are available?
Many patients require no treatment at all. Palpitations can often be treated with medicines or tablets. Sometimes we become more concerned about palpitations and will suggest that you have an electrophysiological catheter study. This is a very sophisticated ECG recording which we take from the inside of your heart. If you have had a stroke or go particularly blue we may suggest that we close the small hole in your heart with a buttonhole device. If your tricuspid valve is very severely affected, sometimes we operate to replace the abnormal heart valve.
Insurance
It can be difficult for people who have congenital heart disease to get insurance. This can cause problems with travel insurance and also when trying to buy a house or get life insurance. There are some more sympathetic insurers who can be identified and contacted through the Somerville patients association.
Tel: 0800 854759
Website: thesf.org.uk
Pregnancy
If you are thinking about having a baby you should see your cardiologist before becoming pregnant to discuss this. Your cardiologist or specialist nurse will be able to give you advice regarding the best form of contraception to use to avoid getting pregnant. The chance of having a child born with a heart problem is slightly higher than normal because you have a heart problem yourself. Your cardiologist will be happy to discuss this with you.
Endocarditis
All patients with congenital heart disease are at risk of infection in the heart (endocarditis). Such infections may be caused by infections of the teeth or gums. It is important to visit the dentist regularly, but you no longer require antibiotics prior to dental work. Due to the increased risk of infection we would also advise against body piercing and tattoos.
• If your tricuspid valve is leaking the surgeon may repair the valve by separating tethered valve leaflets, closing holes in the leaflets and by reshaping the valve leaflets so that they can make contact with each other and prevent backward flow.
• Repairing the valve can involve the surgeon reducing the size of the valve opening and allowing the existing valve leaflets to come together to work properly. A ring may be placed around the valve to support it. This is referred to as an annuloplasty.
• In the case of Ebstein’s anomaly another surgical approach is called the ‘Cone procedure’. This involves the surgeon separating the leaflets of the tricuspid valve from the heart muscle. The leaflets are then rotated and reattached creating a cone from the existing valve leaflets. The cone procedure also involves reducing the area of thinned wall of the right ventricle.
The valve may need repairing again in the future or it may need replacing. Tricuspid valve replacement is less common and surgeons prefer to repair the heart valve rather than replace it when possible. If the valve cannot be repaired, the surgeon will replace the valve by removing the existing valve and inserting a tissue valve.
The Operation
Surgery involves opening the chest through the breast bone and taking over the function of the heart and lungs with a machine (“heart bypass”) to allow the surgeon to stop the heart, and repair the damaged valve. Once the repair is done a scan will be performed to check the valve function. If the surgeon is not happy with the repair he/she will replace the valve whilst still in theatre. At the end of the operation drains are placed into the chest. Pacing wires are also placed on the surface of the heart in case of a low heart rate (bradycardia) in the early post-operative stage. Once the operation is completed the heart bypass machine is turned down and your own heart starts beating by itself. Once the surgeon is happy with your progress the heart bypass machine is removed. The final stage of the operation is to close the chest. Your breast bone is held together with about stainless steel wires and the muscle and skin are stitched. The chest drains are usually removed within 24-36 hours, and the pacing wires after about 4-5 days.
There is a small risk of brain damage (stroke) & death with this procedure. Other problems can occur, such as bleeding, infection, fluid collecting around the heart or temporary electrical instability but these are rarely serious. After surgery a short stay on the intensive care unit (usually overnight) and then a period in hospital for observation (usually about 7 days) is required before going home. Opening the front of the chest leads to a scar and the chest wall will be sore whilst it heals. The time taken to get fully back to normal varies from person to person but can be up to 3 months.
After the Operation
After your operation you will be closely monitored by both the surgeon and cardiologist. A nurse specialist will visit you on the ward and provide you with discharge. The nurse will phone you at home in the week following discharge to check on your progress. You will be given a telephone number that you can contact should you have any concerns in between discharge and follow-up. The team’s physiotherapist can provide exercise plans. These are useful as it is important for your recovery to remain active after the operation.
Final Points
In the 2 weeks leading up to your surgery, you will receive an appointment to come to see the nurse at the pre-admission clinic. This is to make sure that you are fit for surgery and also to give you an opportunity to ask any questions or find out more about coming into hospital.
As for all valve patients, dental work should be completed within 3-6 months before your surgery.