Teen
- About
- Meet The Team
- Conditions
- Aortic Stenosis
- Atrial Septal Defect
- Coarctation of the Aorta
- Complete Atrioventricular Septal Defect
- Interrupted Aortic Arch
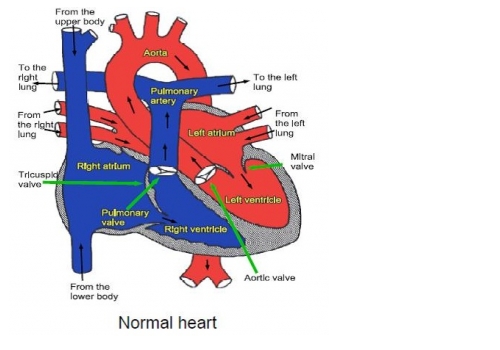
- Normal Heart
- Partial Atrio-Ventricular Septal Defect
- Patent Ductus Arteriosus
- Pulmonary Atresia with Intact Ventricular Septum
- Pulmonary Atresia with Ventricular Septal Defect
- Pulmonary Stenosis
- Small Ventricular Septal Defect (Muscular)
- Small Ventricular Septal Defect (Perimembraneous)
- Tetralogy of Fallot
- Transposition of the Great Arteries
- Ventricular Septal Defect (Large)
- Transition to Adult Congenital Cardiac Services
- Coming in to Hospital
- Surgery and Managing Your Discomfort
- Cardiac Catheter
- Ablation Procedure
- Pacemakers
- Looking after your oral health
- Lifestyle and Exercise Advice
- Periods, contraception and pregnancy
- Support
- Your Views
- Confidentiality and Consent
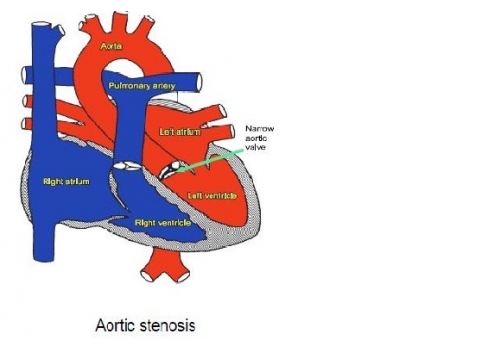
Aortic Stenosis
Aortic stenosis is a narrowing of the valve letting blood flow from the heart to the artery feeding the body with blood (the aorta). Almost all patients with aortic stenosis will need major heart surgery at some stage in their life, but the age at which surgery is necessary is very variable. If the valve is severely narrowed treatment may be necessary within the first few weeks of life, but if the narrowing is slight treatment may not be necessary until later in adult life. The timing of treatment depends on how badly narrowed the valve is, how it changes as time goes by (it almost always gets worse with increasing age), and how well the heart is coping with the extra work of pumping blood through the narrow valve.
When the aortic valve is narrow the muscle of the main pumping chamber of the left side of the heart (the left ventricle) has to work harder than normal and the muscle gets thickened, just like other muscles in the body if they are worked hard. If the valve is only mildly narrowed the heart copes very well, but if the narrowing is very severe the heart cannot pump normally and this can limit how much exercise a patient can manage and can even cause death if it is not treated.
Tests
Usually only simple tests such as an ultrasound scan of the heart (“echocardiogram”) electrical recordings of the heart’s activity (electrocardiogram or ECG) and Xray pictures of the chest are needed to make a diagnosis.
Treatment
Most patients with aortic stenosis will need an operation to replace the valve at some stage, but avoiding this during childhood if possible is the best option as valves do not grow and repeated operations would be needed to put a larger valve in place. When the valve is badly narrowed in childhood we can usually help to delay valve replacement by stretching the narrow valve open with a balloon (called “balloon valvoplasty”).
This is done under general anaesthetic and involves passing a long tube with a collapsed balloon on the end of it (a balloon catheter) into the artery at the top of the leg (or the arm in babies) and feeding it up into the heart and across the narrow valve. Using Xray pictures, the balloon is positioned in the narrow valve and is blown up, stretching the valve open. This never makes the valve normal and it is not always successful, but in many cases it can reduce the severity of the narrowing so surgery can be put off until the patient is older. However it can also make the valve leak which may necessitate valve replacement. Sometimes balloon valvoplasty can be repeated as the patient grows to further delay the need to replace the valve. Usually only one night’s stay in hospital is necessary after the balloon procedure.
If the valve cannot be stretched open using a balloon, open heart surgery will be needed. This involves opening the chest (usually in the middle at the front) and the function of the heart and lungs are taken over by a machine so the surgeon can open the heart and cut the narrow valve open (called a “valvotomy”). Usually about a weeks stay in hospital is necessary after surgical valvotomy.
Sometimes the valve needs to be replaced. There can be two options.
Metal Valve Replacement
One option is to replace the aortic valve with an artificial metal one, because they last longer. Following a metal valve replacement, a drug called warfarin, will need to be taken to reduce the risk of a blood clot forming across your metal valve.
Ross Procedure
Another option for surgery is to use an animal or human tissue valve. This is called the Ross Procedure. The pulmonary valve replaces the narrowed aortic valve, then a ‘tissue valve’ (usually from a pig, or a human valve) is used to replace the pulmonary valve
All treatment for aortic stenosis has potentially serious risks for the patient. Balloon valvoplasty and surgical valvotomy both carry a risk of death (about 1 in 100 in children but higher in very young babies) as well as a small risk (also about 1 in 100) of stroke or other forms of brain damage. Stretching or cutting the valve open helps to reduce the narrowing but almost always makes the valve leak.
General advice for the future
Regular checkups in the outpatient clinic are very important even if the patient appears perfectly well.
Unless the valve is only slightly narrowed, it is usually best to avoid really competitive sporting activities. In most cases swimming, PE, football, netball and similar sports can continued to be enjoyed but more intensive exercise such as cross country running and squash should be avoided. Your cardiologist will answer any questions you have about individual recommendations for you or your child.
Patients with aortic stenosis will be at risk of infection in the heart (called endocarditis), both before and after treatment. Such infections may be caused by infections of the teeth or gums. It is important to visit the dentist regularly (every 6-12 months) and to follow good dental hygiene. Ear or body piercing and tattooing are best avoided as they also carry a small risk of infection which may spread to the heart.