Adult
- About
- Meet The Team
- Conditions
- Anticoagulation in Pregnancy
- Aortic Dilatation and Pregnancy
- Aortic Valve Disease
- Aortic Valve Replacement
- Atrial Septal Defect
- Coarctation - Transcatheter stent (keyhole) treatment
- Coarctation of the Aorta
- Congenitally Corrected Transposition of the Great Arteries
- Ebsteins Anomaly
- Eisenmenger’s Syndrome
- Fontan Circulation
- Mitral Valve Repair/Replacement
- Normal Heart
- Patent Foramen Ovale
- Pregnancy information for women with metal heart valves
- Pulmonary Incompetence
- Pulmonary Stenosis
- Pulmonary Valve Replacement - Surgery
- Pulmonary valve replacement - Transcatheter (keyhole) treatment
- Repaired Atrioventricular Septal Defects
- Sub-aortic Stenosis
- Surgical treatment of Atrial Septal Defect
- Tetralogy of Fallot
- Transposition of the Great Arteries - The Atrial Switch (Mustard or Senning) procedure
- Transposition of the Great Arteries – Arterial Switch
- Ventricular Septal Defect
- Ventricular Septal Defect - Transcatheter (keyhole) treatment
- Patient Feedback
- Making the most of your clinic appointment
- Your Appointment in Outpatients
- Easy Read Guide for Out Patients
- Cardiac Catheter
- Transoesophageal Echocardiogram
- MRI
- Surgery & "Top Tips" for coming into hospital
- Lifestyle Advice
- Exercise
- Heart Failure
- End of Life and Palliative Care
- Looking after your oral health
- Dentists Information Section: Dental care in adults at risk of Infective Endocarditis
- Yorkshire Regional Genetic Service
- Support
- Video Diaries
- Second Opinion
- Monitoring Results at Leeds Infirmary
- Professionals
Mitral Valve Repair/Replacement
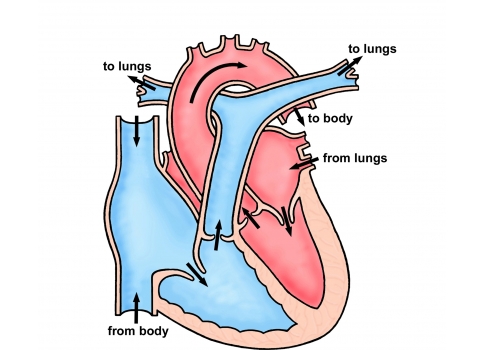
The mitral valve is located on the left side of the heart between the atrium and the ventricle. Blood returning from the lungs (where it picks up oxygen) enters the left atrium (collecting chamber) and then into the left ventricle (pumping chamber) from where it is pumped to the rest of the body. The function of the mitral valve is to ensure that blood travels in one direction and does not leak back to the lungs.

In some cases, the leaflets of the mitral valve can be abnormal. Valve leaflets can be thickened causing the valve to be narrowed. The medical term for this problem is mitral stenosis. If the valve leaks then the medical term for this is mitral regurgitation. In some cases individuals have a combination of mitral stenosis (narrowing) and mitral regurgitation (leak). Mitral valve disease causes the heart to work harder in order to push the same amount of blood forward and over time the pump will become less efficient and the heart may begin to fail.
Tests
The Operation
Mitral valve disease (leak or narrowing) can be treated by an operation in which the valve is replaced. The operation is always performed under a general anaesthetic so you will be asleep. The surgeon makes an opening in the middle of the chest through the breast bone to get to the heart. During the operation, the function of the heart and lungs is taken over by a machine (“heart bypass”). The surgeon can then stop the heart and remove the damaged valve. In some cases the surgeon will attempt to repair the valve instead of replacing it. The risk of death for repairing the valve is 1-2% versus 4-5% for replacement. If repair is not possible, then a new replacement valve will be sewn in place. After the operation the breastbone is closed using stainless steel wires and surgical drains (tubes) are positioned in the chest to allow any excess fluid to drain. These are normally taken out after about 24 hours. As a precaution, pacing wires are placed on the surface of the heart in case of a low heart rate (bradycardia) in the early post-operative stage, these are removed 4-5 days after the operation.
There are 2 types of valve which are commonly used:
Tissue Mitral Valves — engineered from a pig or cow heart valve. The main advantage to tissue valves is you don’t have to take Warfarin (blood thinners) but the disadvantage is that it only lasts 10-15 years.
Mechanical Mitral Valves — made from metal. You would need to take Warfarin tablets for life afterwards. This can be very important if you are a woman and thinking about having a family in the future due to the side-effects of the medication and effects on an unborn child. The main advantage of having a metal valve replacement is that it should last for many years and possibly forever.
There is a small risk of death and a very small risk of major complications such as brain damage (1 in 100). Other complications such as bleeding, infection, fluid collecting around the heart or lungs can occur after the operation but these are rarely serious, although they may need treatment. After surgery a short stay on the intensive care unit (usually overnight) is required. You will then remain in hospital for further monitoring of your recovery. This is usually for about 7 days but can be longer. Opening the front of the chest leads to a scar and the chest wall will be sore whilst it heals. The time taken to get fully back to normal varies from person to person but can be up to 3 months.
Tests
After the Operation
After your operation you will be closely monitored by both the surgeon and cardiologist. A nurse specialist will visit you on the ward and provide you with discharge advice. The nurse specialist will phone you at home in the week following discharge to check on your progress. You will be given a telephone number that you can contact should you have any concerns in between discharge and follow-up. The team’s physiotherapist can provide exercise plans. These are useful as it is important for your recovery to remain active after the operation.
Final Points
In the 2 weeks leading up to your surgery, you will receive an appointment to come to see the nurse at the pre-admission clinic. This is to make sure that you are fit for surgery and also to give you an opportunity to ask any questions or find out more about coming into hospital.
It is also important to make sure that all dental work has been completed within 3- 6 months prior to your surgery and that you are informed of the contraindications to Warfarin so that the right type of valve (metal or tissue) can be chosen for you.